


Donor Disparity
Could value-based bone marrow transplants accelerate the timeline to successful treatment?

Bone marrow transplants, while usually a last-resort treatment, are often curative and life-changing. However, for allogeneic bone marrow transplants where the donor is unrelated to the patient: the patient must find a matching bone marrow donor. A match allows a pediatric patient with Acute Lymphoblastic Leukemia (ALL) to essentially be cured, rather than suffering a long and painful life of chronic transfusions to replenish their immune agents.
Unfortunately, there’s a huge shortage of registered bone marrow donors from minority backgrounds. Despite the amazing work by organizations like Be The Match, who actively campaign to grow the National Marrow Donor Registry (NMDP), there’s an especially large disparity of registered Black donors. Black patients only have a 22% chance of finding a match through NMDP, compared to 77% for whites (more details from this study). For patients of mixed ancestry, the likelihood of finding a match drops precipitously - only 4% of the registry are of mixed race backgrounds.

One of the many underlying issues at play is historical and current distrust of medical institutions by minority communities. This mistrust is fueled by many examples, including the infamous Tuskegee experiment where Black men with syphilis were denied life-saving medical care for decades; this mistrust is continued today, as providers continue to systemically under-treat Black Americans for pain.
The resulting disparities in the donor pool lead to statistically significant differences in survival for aggressive conditions like Acute lymphocytic leukemia, especially for younger patients where earlier intervention is particularly important for being potentially curative.

Five-year relative survival for patients with ALL by age group and race from SEER 18 (2000-2014). Non-Hispanic whites were used as the reference group. Hispanic categorization was not mutually exclusive from other race categories.17 Reported data used unadjusted P values. **P < .001; *P < .05. PLOS Study
Behind these statistics are so many heartbreaking stories of patients who wait years on the donor list and end up passing due to complications from waiting for too long. Two examples are shown below:

Destiny Worthington has had continuous transfusions for over a decade due to her aplastic anemia

Jennifer Jones Austin who ultimately never found a match, but through her inspiring personal campaign through Black Bone Marrow enrolled 12K+ donors into NMDP
Challenges
In a lot of these stories, the campaign to find a compatible match ends up being the onus of the patient and their personal support system. Patients are known to have better outcomes when they receive treatment and transplantation earlier, yet they often receive minimal support in launching these campaigns. The costs of the donor search unfortunately only add to the financial and physiological tolls that patients incur from the continuous transfusions they receive and the increasing complications due to these chronic conditions. Many patients and their families are ultimately bankrupted by the incredibly high costs of co-pays and medications that these conditions end up causing.
A common response to the is a focus on increasing donor registration across the US population. Unfortunately, even the significant efforts to increase the donor pool may do little to move the needle on match success rates.
Challenges with Increasing Donor Diversity
Probably the most counterintuitive learning is that significantly increasing the donor diversity in the NMDP registry will not ultimately move the needle that much on successfully matching a minority patient. Though I won’t dive into HLA population genetics, the rapidly growing diversity of the US population seems to be outpacing the amount of donors we can feasibly add to the donor pool. According to a former transplant director I spoke to, “The problems of donor search are those of linkage disequilibrium - even if every African American was in the registry we would still not find donors as the same rate of other populations”.
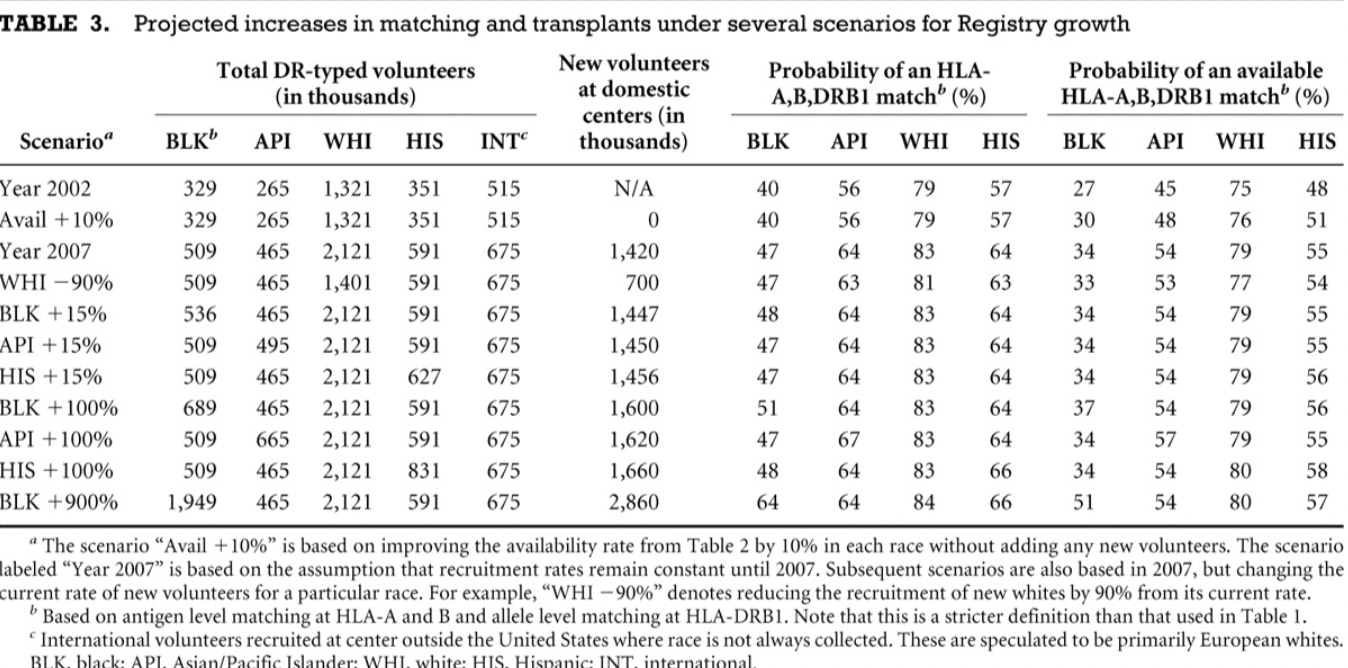
For research looking into this issue, consider the following quote and table from this paper which also suggest that improving donor retention and patient access to the registry may be more cost-effective than adding new volunteer donors:
Continued recruitment of additional volunteers can provide HLA-matched donors for more patients, but the models developed in this study predict that disparities between racial/ethnic groups will still exist. Doubling the recruitment rate of new minority volunteers only increases the projected likelihood of finding an HLA-matched donor by a few percent. Adding 2 million more black volunteers, which would be six times the current number on the NMDP Registry and represent approximately 15% of blacks in the entire U.S. (19), would still result in a predicted match rate for patients of that ethnicity lower than the year 2002 level for whites.
On the Horizon: Haplo and Cord Blood Transplants
On the upside, there are a number of emerging alternative donor transplant options like haplo donors (guaranteed half matches from parents/siblings) and cord blood (collected from the umbilical cord after birth) for underrepresented minorities who can’t find a matching donor for an allogeneic bone marrow transplant. In recent years, advances around these alternative transplantation procedures and specifically research in post-transplant medications have mitigated the risk of rejection of donated stem cells (graft-versus-host disease).
Coordination: The Ignored Bottleneck
Despite these advances in care, there are incredible coordination challenges and payer-provider disincentives that prevent patients from getting timely transplants. Because most transplant centers exist only in tertiary care centers, almost all patients have to go through this complicated referral pathway. Coordination between rural and academic centers are incredibly labor-intensive and associated with a number of non-clinical costs that commercial and Medicaid insurers may not cover.
In my opinion, this is the more important and practical bottleneck that can improve the outlook for patients who need bone marrow transplants - especially underrepresented minorities who have trouble finding an allogenic match.
So how can we better align incentives to improve coordination between referring and receiving providers? And more importantly begin shifting the onus of this responsibility away from our patients?
An Idea: BPCI Advanced Model for Bone Marrow Transplants
For folks new to alternative payment models, Bundled Payments for Care Improvements (BPCI) is an experimental model designed by CMS/CMMI that aims to align incentives among participating health providers around a set of specific clinical episodes. To participate, you typically need some sort of convener participant that can facilitate coordination to bear and apportion financial risk of the participating providers.
I wonder if there’s an opportunity for a convening entity to be created that can help align referring and receiving providers. With allogeneic bone marrow transplants being one of the costliest medical procedures (~$800K for allogeneic transplants) in the country - second only to liver transplants, there could be significant financial cost-savings shared in a well-coordinated convening entity. This type of organization and payment model could also better incentivize the important follow-up (e.g., chronic GVHD therapy, infection management) and complex transitions of care between different institutions. Moreover, there would be incentives aligned across referring and referral providers to help patients get the life-saving treatment they need earlier in an effort to drive costs down collectively.
This model would help build on the Oncology Care Model proposed by CMS which allows providers to receive a performance-based payment for enhanced care coordination but perhaps be better tailored to the large variation in high-cost drug therapies and provide more centralized services shared across referring/referral institutions through a convener entity.
In order for this model to be effective, there would have to be clearly demonstrated cost-savings or clinical quality measures that could incentivize earlier treatment of bone marrow transplant when compared to the longitudinal expenses of continuous treatment and increasing chronic conditions. But I’d love to hear your thoughts below on shortcomings in this type of model and thoughts on what other approaches should be considered!
Huge thanks to Dr. Gunjan Shah for pointing me to many helpful articles in researching this topic and Dr. James Gajewski for his thoughtful feedback throughout. Grateful also to Dr. Eileen Scigliano and Dr. Adriana Malone for educating me about alternative donor transplant options. Big thanks also to Juliana, Jared, and Terrance for some incredibly helpful edits in refining this post.
There’s a lot that this post went over and a number of ideas I edited out (e.g., single payer system for transplants, digital-first donor drive efforts) that I’d love to share with anyone interested in continuing this thought exercise. As always, encourage folks to fill out the below form if you’re interested in connecting with other readers in diving into any of the above or collaborating on future topics/posts.