


Thrombectomy Coordination and Stroke Therapy,
How can technology be used to improve accessibility to acute and recovering stroke patients?

[Viz.AI: LVO Suspected]

We saw the notification pop up and started reviewing the imaging on a patient anticipating the stroke code that would be called minutes later. Rushing downstairs, I replayed the clinical symptoms of aphasia, contralateral hemiparesis we would be suspecting from the large left MCA infarct we saw scrolling through the Viz AI mobile app. Gathering history from the EMTs that brought the patient in from a nearby nursing home, we learned the last known well for the patient was within the 4.5h window for the clot-dissolving medication tPA. We worked quickly with the EM physicians to determine if the patient was a candidate for acute intervention - I called the nursing home to learn if the patient was on any anticoagulation therapy, the EM intern looked through the chart to find a family contact who could confirm the patient’s code status, and the rest of the stroke team started consulting with our attending and confirming the clinical findings on neurological exam.
Minutes later, we got the final read of the CT scan from a neuroradiologist and had consulted with our senior stroke attending. Given the findings of older subacute strokes in the patient, we decided sending the patient emergently across town for thrombectomy would lead to a better outcome. Since the Viz AI notification had fired across all of the Mt Sinai hospitals, the endovascular neurology fellow was already primed to receive the details of the case for which we were already coordinating transfer.
As a longtime admirer of Viz AI as a former machine learning researcher and digital health VC, it was inspiring to see how technology was coordinating these specialized teams in real-time while a medical student on the stroke service. As smoothly as this case went, enabled by the Viz AI technology and coordination to detect stroke candidates for acute intervention - I couldn’t help but think about how this scenario would have played out in a region of the US that lacked accessibility to the many tiers of expertise and triage that happened in under an hour at our Mt Sinai hospitals.
Stroke Centers

There are four tiers for Stroke centers as defined by the Joint Commission in collaboration with the American Heart Association. Pre-admission triage by Emergency Medical Service (EMS) technicians dictate the level of stroke center to which a stroke patient will be routed; considerations include severity of the symptoms, evaluation of the level of medical care that may be needed, and the relative distance of various certified stroke centers in the vicinity of each medical event.
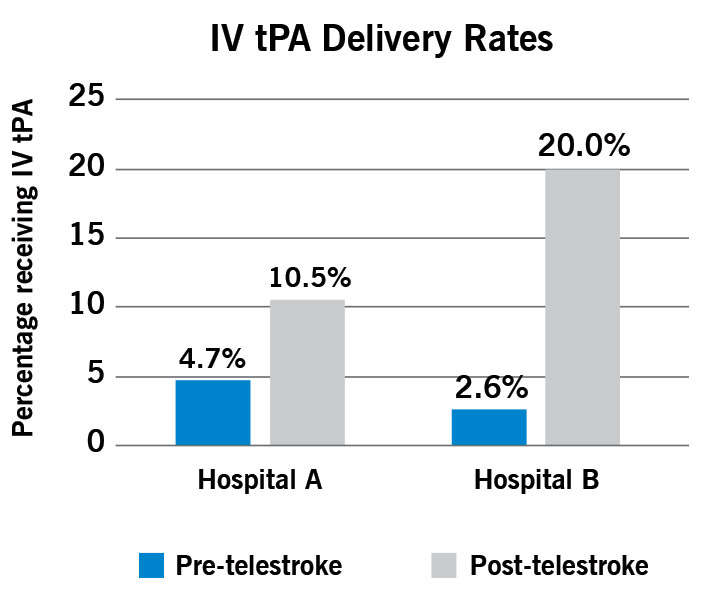
Launched in 2011, the Cleveland Clinic Telestroke Network (CCTN) created a hub-and-spoke model partnering with “spoke” facilities around the hub of Comprehensive Stroke Center on Cleveland Clinic’s main campus. When patients identified with stroke arrive at the emergency department (ED) of a partner facility, emergency physicians perform a rapid assessment, order a CT scan and then call the CCTN. A CCTN stroke neurologist works remotely with the ED staff to check vital signs, perform a neurological examination, review results of the CT scan and make treatment decisions.
Since its inception, the CCTN has grown to support 15 hospitals and freestanding EDs that do not have stroke specialists - eight within the Cleveland Clinic health system and seven external facilities across Ohio, Pennsylvania, and Florida.
There are even mobile CT-equipped EMS vehicles that allow CT imaging to be done wherever the patient is and real-time remote examination of stroke patients alongside a stroke-trained nurse who can administer TPA. The study showed a reduction of image availability in PACS (the hospital-based radiology system) by 41 minutes from 97 to 56 minutes. The MSU facilitated provision of actionable reports within 60 minutes of dispatch, the so-called “golden hour,” in 100% of patients compared with only 78% in the control group.
Disparities in tPA Administration

Overall, only about a quarter of stroke patients arrive within the 4.5h window in which tPA can be administered, and only 2-5% of all stroke patients in the US ultimately receive tPA after ruling out contraindications or delays in provider assessment. However, studies have shown that racial disparities exist in tPA administration - that Black patients were one third less likely than whites to receive IV tPA (3% vs. 10%, p<0.001). Even when presenting within 3 hours (enough time to activate a stroke code and obtain imaging), Blacks were almost 50% less likely to be treated with IV tPA than whites (27% vs. 46%, p=0.023). Whether this is due to provider bias or systemic barriers that prevent Black patients from getting evaluated and treated in a timely manner, perhaps technologies like Viz AI can help facilitate much more timely and equitable decision-making based on demonstrable findings on CT imaging.
Idea: Coordinating Thrombectomy Referrals
One of the issues with Viz AI is that it requires primary stroke centers to buy into a subscription model and ultimately lose patients through direct referrals to more comprehensive centers. This introduces some barriers especially to more rural areas that are outside of the academic medical centers that can afford and implement the Viz AI integration given the diversity of both primary and comprehensive stroke centers in a larger system. Though Medicare has tried to offset this by allowing these hospitals to be reimbursed through its New Technology Add-On Program, the financial incentive for out-of-network primary stroke centers to buy into a network and integrate this software is thin.
What if we could create a venture that helped streamline the coordination and referral of patients directly to a thrombectomy center if clinically appropriate? A venture that owned and built out a fleet of mobile-equipped EMS vehicles equipped with its own remote stroke physicians (neuroradiologist, stroke neurologist), and stroke-trained staff could potentially direct thrombectomy-eligible patients to a comprehensive stroke center directly without an initial assessment from a primary stroke center. Partnering stroke hospitals would benefit from the increased thrombectomy cases they receive and early activation through real-time integration with the mobile CT scanner.
The question then becomes, how to activate such a service - the venture would have to integrate into 911 call center triage workflows to learn from trigger phrases like “slurred speech” “face feels droopy” and other clinical signs that would key an EMS provider into a stroke assessment.
Related ideas:
One idea to help bridge the gap between primary and comprehensive stroke centers is for Viz AI (or a separate venture that licenses Viz AI) to provide tech-enabled services (e.g., a remote neuroradiologist and stroke attending) for free to primary stroke centers and share in the reimbursement from successful thrombectomy referrals/procedures. This venture could build integration hooks into the PACS systems at these primary stroke centers and deploy a remote team to kick off the transfer/triage decision to partnering comprehensive centers. Similar to how the Mt Sinai stroke team works, a fellow can monitor Viz AI and begin activating a center for thrombectomy if the patient qualifies.
This model could be tied to RVUs captured by turning some hospitals into “acute stroke-ready hospitals” and streamlining transitions of care (see Lessons Learned from Mayo Clinic’s Redesign of Stroke Care) at higher-level stroke centersStudies have also proposed the combination of transcranial ultrasound and clinical assessment to diagnose ischemic stroke in rural settings - I wonder if anyone has tried to deploy ultrasound in the field to help decouple the need for the non=contrast CT scan.
Idea: Tele-Speech Therapy
Inspired by another patient I worked with who had a left MCA territory infarct that led to aphasia (loss of ability to understand or express speech) and word-finding difficulty but spared any motor or sensory deficits. Up to a third of stroke patients experience aphasia but not all of these patients have severe enough physical impairments that would necessitate physical therapy. From an insurance standpoint, these patients are caught in the middle because they do not qualify for in-home services that come 3-4x/week. Unless in-home physical or occupational therapy is deemed medically necessary, patients will often have to set up their own outpatient speech therapy that only meets 1/week.
High quality speech and language therapy that is delivered over video conference could help meet the gap for patients, especially those who would have trouble getting to/from their outpatient therapy appointments. Though online speech therapy companies exist (e.g., Stamurai, Expressable) most seem to focus on language developmental challenges in early childhood and do not seem specialized in helping adults recover from strokes. These companies also don’t seem to accept insurance which would likely consider aphasia from a recent stroke medically necessary.
I forgot I had this draft saved from January but a belated big thanks to Dr. Kurt Yaeger (our Chief Neurosurgery Resident) and Dr. Vineeth Gangaram for their thoughtful comments on early drafts of this piece. Grateful for the Mt Sinai Morningside Stroke Service - especially our site director Dr. Joseph Diamond who I had the privilege of working with during his last week on service before starting his new job at Northwell
Would love to hear feedback and comments from folks who have worked with stroke patients or want to riff on some of the ideas posed here - always open to your thoughts!
Thinking more about the most effective ways mobile CT unit can be deployed to the field after a paramedic/EMT evaluates and confirms that it's a true stroke. The use case of doing a scan in the field and being able to triage on the fly whether a LVO can be treated with TPA or the vehicle can skip a community hospital and go straight to a thrombectomy center